Most defensive shooters know the cardiac box as the default shot. Fewer can describe the moment they should stop taking it. The shift from cardiac box to cranial T-box is not a textbook switch — it is a real-time read of the threat presentation, made under stress, against a target that is moving and changing geometry as the engagement unfolds. The shooter who has trained that decision lands the shot. The shooter who has not freezes, takes a denied shot, or hits a hostage.
The shift between these two anatomical zones is what separates competent defensive shooting from drill marksmanship. It is also one of the most under-trained skills in the CCW curriculum.

The cardiac box: the default for a reason
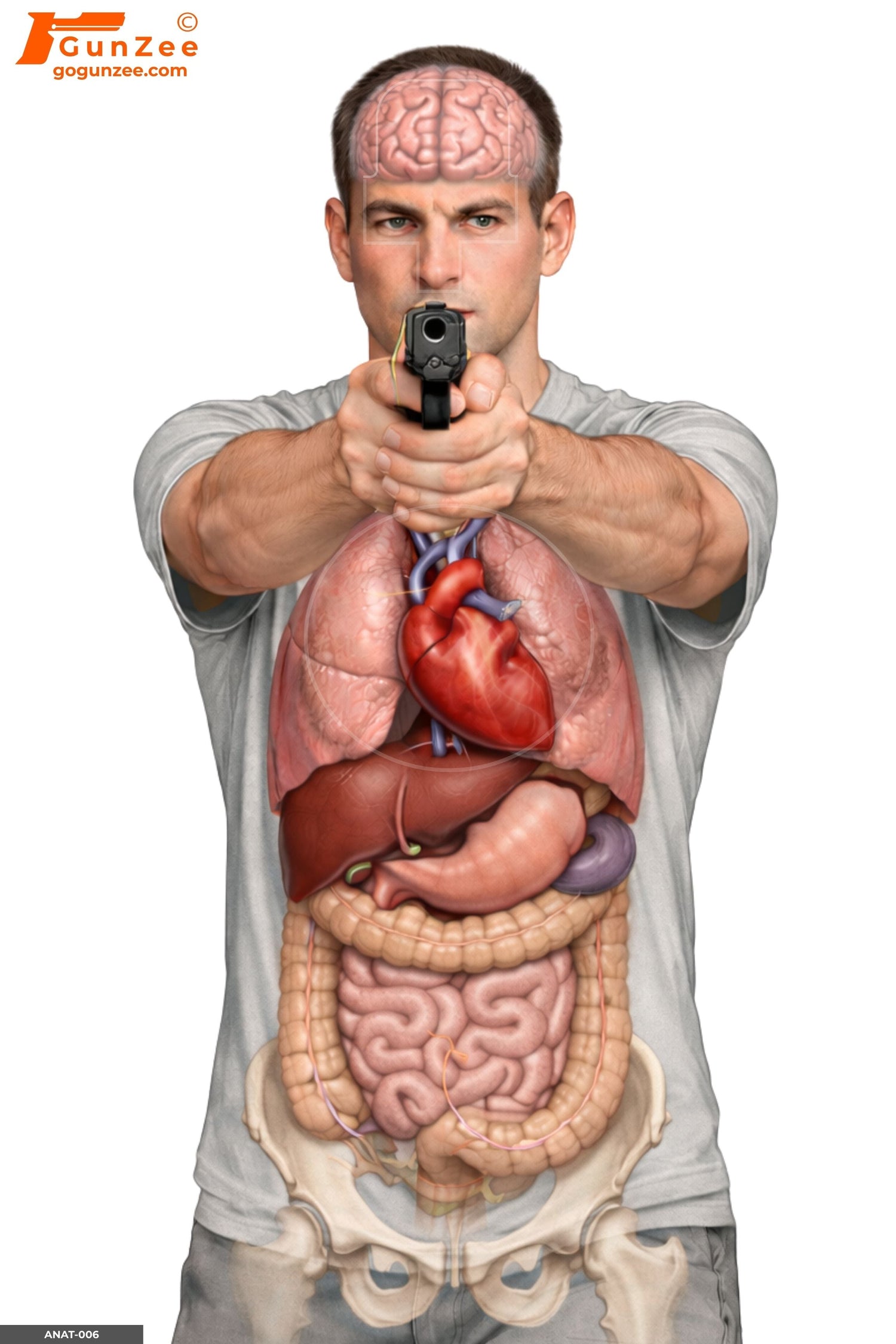
The cardiac box is roughly a four-by-four-inch area centered between the nipples, covering the heart, the great vessels of the upper thorax, and the upper lobes of the lungs. A hit causes rapid blood-pressure collapse and ends most fights in seconds rather than minutes. It is the highest-probability stop zone for handgun rounds, the largest reliable target on the threat's body, and the shot that requires the least precision.
That last property is what makes it the default. Under stress, accuracy degrades. The cardiac box is wide enough to absorb that degradation and still stop the fight. Almost every defensive curriculum starts here for a reason — and almost every shooter spends the bulk of their range time training this single placement on an Anatomical Full-System Vital Zone target or the Anatomical Frontal Handgun Threat target.
This is correct. It is also incomplete.
The cranial T-box: the answer when cardiac is denied
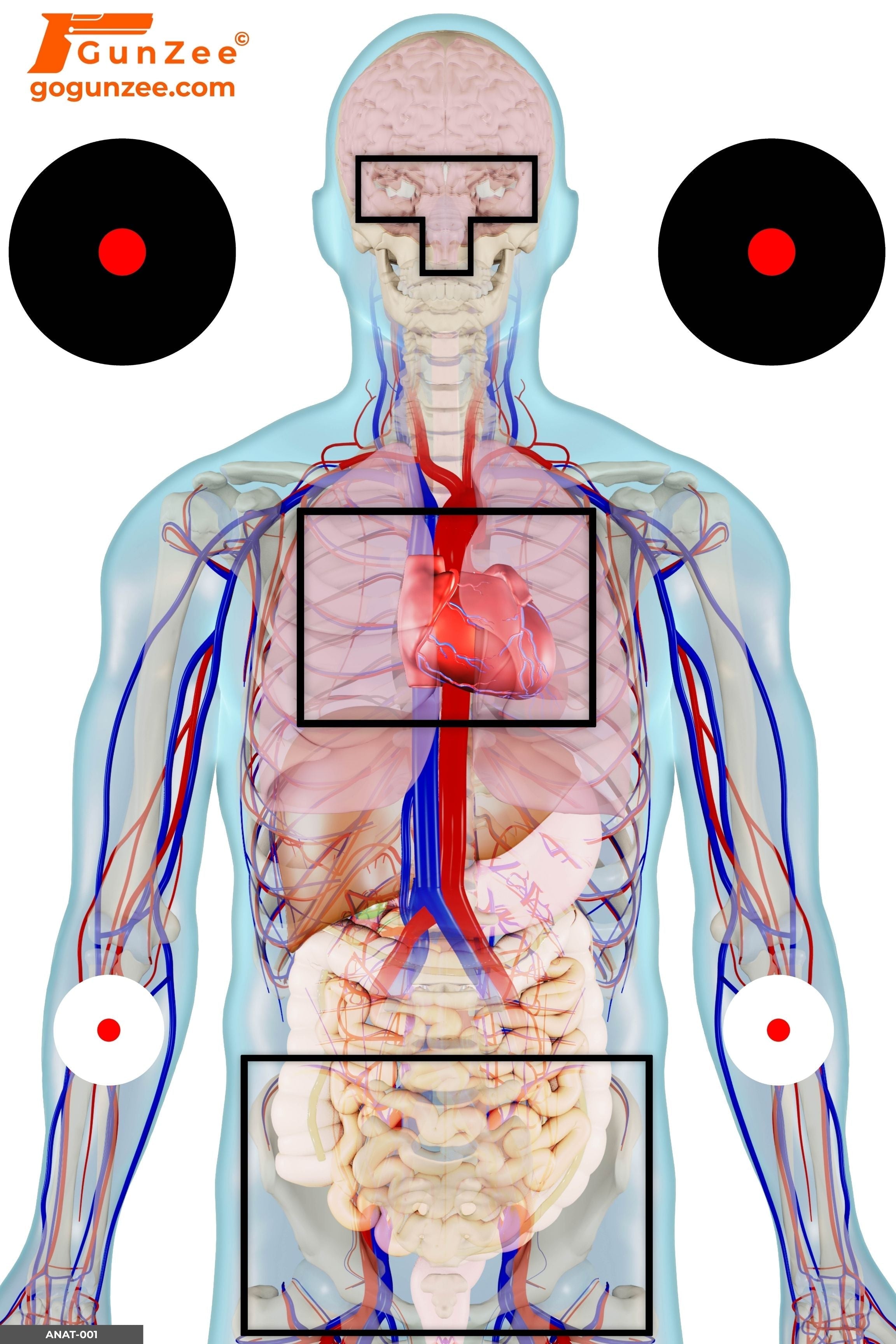
The cranial T-box is the T-shaped zone formed by the horizontal line across the eyebrows and the vertical line down the bridge of the nose to the upper lip. The T runs roughly two inches wide at the eyes and four inches tall at the vertical bar. A hit anywhere inside this T reaches the brainstem and produces an instantaneous stop — no delayed collapse, no muscular response, no continued trigger press on a hostage. The threat goes off like a switch.
That instantaneous-stop property is what makes it the answer in three specific situations:
- Hostage interposition. A hostage's body blocks the cardiac box; only the T-box remains as an ethical shot. This is the textbook hostage-rescue scenario and the most-discussed application.
- Body armor. A threat wearing rifle-rated plates defeats cardiac box rounds. The T-box bypasses the armor entirely.
- Imminent trigger press on a non-threat. The threat has a weapon presented at a hostage or a third party. A cardiac box shot will stop the fight but may not stop the trigger finger before the cardiac collapse takes effect — that takes seconds, and seconds are enough for the threat to fire. T-box removes the muscular response and the trigger press together.
The shift: when to move from cardiac to T-box
The shift is a visual decision made in real time. Specific cues that should trigger it:
The hostage geometry. A hostage moves between the shooter and the threat — even partially — and the cardiac box footprint shrinks or disappears. The Anatomical Hostage Shield target trains exactly this geometry: the threat's cardiac box is occluded behind the hostage's torso and only the T-box remains visible above the hostage's head.
The armor visible on the threat. Rifle plates show as a flat panel across the chest with characteristic edges or carrier straps visible. When the shooter reads armor, the cardiac box is no longer reliable; T-box becomes the only stopping shot.
The hostage at gunpoint. The threat's weapon is presented at a non-threat — finger on the trigger, muzzle on the hostage. The cardiac box shot will succeed eventually; the T-box shot will succeed immediately. Seconds matter.
Profile and semi-profile angles. At a true profile, the cardiac box is no longer a four-by-four-inch box — it is a thin vertical column the width of the heart, and the lung tissue around it is mostly air. The Anatomical Semi-Profile target and the Anatomical Semi-Frontal target show how the cardiac box compresses at angles, and at some point the T-box becomes the larger and more reliable target.
What "training the shift" actually looks like
The shift cannot be drilled by repeating cardiac box shots and hoping T-box ability shows up under stress. The shift is its own skill. A useful progression for a CCW holder building it:
- Establish cardiac box reliability first. Two-inch groups at 7 yards on a reference target before adding T-box work at all. If the cardiac box is not consistent at distance, T-box practice is wishful thinking.
- Add isolated T-box reps. Same target, same distances, T-box only. Expect a measurable accuracy drop. The T-box is smaller; the head moves more; the structure is harder. Most shooters need 200 to 500 reps before T-box hit rate stabilizes at 7 yards.
- Practice the shift on a hostage target. The Anatomical Hostage Shield target forces the decision: the cardiac box is denied, the T-box is the answer. Draw, present, identify the geometry, take the T-box shot. The "identify the geometry" beat is the part most range drills skip.
- Add angle work. Rotate through the semi-frontal and semi-profile anatomy targets. The decision to shift sometimes flips earlier than the shooter expects because angle changes degrade cardiac viability faster than range time reveals.
- Add scenario integration. Once the placement decision is reliable, fold it into scenario drills with multiple targets and decision pressure. This is where scenario targets like the CQB Hostage Forward Weapon Presentation target and the Corridor Hostage Control target earn their place — they present the cardiac/T-box decision inside an environment, not in isolation.
Common errors that kill T-box reliability
Practicing T-box only with deliberate, slow fire. The T-box shot in reality is taken at speed. Slow-fire T-box practice teaches a placement the shooter cannot replicate under stress. Mix speed early.
Aiming at "the head" instead of the T. The head is bigger than the T-box and a head hit outside the T-zone is not a stopping shot — it can deflect off skull, fail to reach the brainstem, or simply wound. A precise mental image of the T, not the head, is what training builds.
Treating the T-box as a backup for missed cardiac. If the first cardiac shot misses, more cardiac shots are usually the right answer — not a T-box transition. T-box is for when cardiac is denied or insufficient, not when cardiac was attempted and failed.
Failing to train the visual identification. The hardest part of the shift is reading the geometry in real time, not making the shot. Range drills that simply tell the shooter "take a T-box shot" skip the actual decision. The shooter has to see the cue and shift on their own.
Where this fits in the broader anatomical curriculum
The cardiac box-to-T-box shift is one specific skill within the larger discipline of anatomical shot placement. The full case for why anatomical training beats silhouette work is covered in Anatomical Targets vs. Bullseye: Why Shot Placement Saves Lives. The breakdown of all eight anatomical targets in the GunZee line and how each one builds a different engagement geometry is in Human Anatomy Shooting Targets: A Complete Training Guide.
The full anatomical library lives in the Anatomical Shooting Targets collection.
→ BROWSE ANATOMICAL TARGETS FOR T-BOX TRAINING
Frequently asked questions
What is the cardiac box?
The cardiac box is roughly a four-by-four-inch area centered between the nipples, covering the heart, the great vessels of the upper thorax, and the upper lobes of the lungs. A hit causes rapid blood-pressure collapse and ends most fights in seconds.
What is the cranial T-box?
The cranial T-box is the T-shaped zone formed by the horizontal line across the eyebrows and the vertical line down the bridge of the nose to the upper lip. A hit reaches the brainstem and produces an instantaneous stop with no muscular response from the threat.
When should a shooter shift from cardiac box to T-box?
When the cardiac box is occluded or unavailable — body armor, hostage interposition, severe angle, or the need for instantaneous stop (a finger already on a trigger pointed at a hostage). The shift is a real-time decision based on what the threat presents, not a textbook switch.
Is the T-box harder to hit than the cardiac box?
Yes. The T-box is roughly two inches wide by four inches tall — significantly smaller than the cardiac box and on a body part that moves more. Reliable T-box hits demand training reps the average shooter has not put in.
What targets train the cardiac box-to-T-box shift?
The Anatomical Full-System Vital Zone target trains the reference geometry. The Anatomical Hostage Shield target trains the shift itself by occluding the cardiac box behind a hostage. The Semi-Profile and Semi-Frontal anatomy targets train the same shift at the angles real engagements present.
Should every CCW holder train T-box shots?
Yes — but only after cardiac box hits are reliable at distance. T-box training before cardiac fundamentals just builds frustration. Once cardiac groups stabilize at 7 to 10 yards, T-box becomes the next layer.
Go deeper: the silhouette-to-realism upgrade path explains why ring-scored outlines hide these aim points, and the defensive shooter’s guide to target types shows where placement work fits in a full rotation. Train it on the full paper shooting targets collection.

{kind=link}